Driving along Reykjavik’s windswept roads on a cold March morning, Kári Stefánsson turned up the radio. The World Health Organization had just announced that an estimated 3.4% of people infected with SARS-CoV-2 would die — a shockingly high fatality rate, some 30 times larger than that for seasonal influenza.
There was a problem with that estimate, however: it was based on reported cases of COVID-19, rather than all cases, including mild and asymptomatic infections. “I couldn’t figure out how they could calculate it out without knowing the spread of the virus,” recalls Stefánsson, who is the founder and chief executive of deCODE genetics, a human-genomics company in Reykjavik. He became convinced that making sense of the epidemic, and protecting the people of Iceland from it, would require a sweeping scientific response.
When Stefánsson arrived at work, he phoned the leadership of Amgen, the US pharmaceutical company that owns deCODE, and asked whether he could offer deCODE’s resources to track the spread of the virus, which had landed on Icelandic shores only six days earlier. “The response I got from them was, ‘For heaven’s sake, do that,’” says Stefánsson.
Over the ensuing nine months, deCODE and Iceland’s Directorate of Health, the government agency that oversees health-care services, worked hand-in-hand, sharing ideas, data, laboratory space and staff. The high-powered partnership, coupled with Iceland’s diminutive size, has put the country in the enviable position of knowing practically every move the virus has made. The teams have tracked the health of every person who has tested positive for SARS-CoV-2, sequenced the genetic material of each viral isolate and screened more than half of the island’s 368,000 residents for infection.
Late nights analysing the resulting data trove led to some of the earliest insights about how the coronavirus spreads through a population. The data showed, for example, that almost half of infected people are asymptomatic, that children are much less likely to become sick than adults and that the most common symptoms of mild COVID-19 are muscle aches, headaches and a cough — not fever. “Scientific activities have been a huge part of the entire process,” says Runolfur Palsson, director of internal-medicine services at Landspitali — The National University Hospital of Iceland. Researchers at deCODE and the hospital worked day in and day out to gather and interpret the data.
Their achievements aren’t merely academic. Iceland’s science has been credited with preventing deaths — the country reports fewer than 7 per 100,000 people, compared with around 80 per 100,000 in the United States and the United Kingdom. It has also managed to prevent outbreaks while keeping its borders open, welcoming tourists from 45 countries since mid-June. The partnership again kicked into high gear in September, when a second large wave of infections threatened the nation.
Careful steps
COVID-19 is not the first pandemic to reach Iceland’s shores: in October 1918, two ships carrying pandemic influenza docked in Reykjavik’s downtown harbour. Within six weeks, two-thirds of the capital city’s inhabitants were infected1.
A century later, the Icelandic government was better prepared, enacting a national pandemic preparedness plan at the beginning of January, two months before COVID-19 arrived. “We decided from the beginning we would use isolation, quarantine and contact tracing,” says Þórólfur Guðnason, chief epidemiologist at the Directorate of Health. As part of that plan, the microbiology laboratory at the university hospital began testing citizens in early February.
On 28 February, a man returning from a skiing holiday in northeastern Italy tested positive for the virus. Within a week, the number of cases had climbed from 1 to 47, the opening notes of a coming crescendo. As health-care workers began ordering hundreds of tests per day, one of the hospital’s machines for isolating and purifying RNA broke from overuse. “We were not able to cope with all the specimens coming in,” recalls Karl Kristinsson, the university hospital’s chief of microbiology.
By 13 March, deCODE had begun screening the general public and was able to quickly take over much of the hospital’s testing. The company repurposed a large phenotyping centre that it had been using to study the genetics of Icelanders for more than two decades into a COVID-19 testing centre. “It almost looked like these 24 years preceding COVID-19 had just been a training session,” says Stefánsson. “We dove into this full force.”

One of the first families in Iceland to be screened with deCODE’s COVID-19 test.Credit: Jon E. Gustafsson
The company has the staff and machinery to sequence 4,000 whole human genomes per week as part of its regular research activities, says Stefánsson. Throughout the spring, it would set that aside to devote its analytical and sequencing heft to the pandemic response.
deCODE’s main activity has been COVID-19 screening, including open invitations to the general population. Today, any resident with even the mildest symptom can sign up to be tested. Residents sign up online using dedicated COVID software built by deCODE programmers. At a testing centre, they show a barcode from their phone to automatically print a label for a swab sample. Once taken, the sample is sent to a laboratory at deCODE’s headquarters that is run jointly by the university hospital and deCODE and operates from 6 a.m. to 10 p.m. Results are always available within 24 hours, but are often ready in just 4 to 6. “We now have the capacity for about 5,000 samples per day,” says Kristinsson. As a whole, the collaborators have so far screened 55% of the country’s population.
If the test is negative, the person receives an all-clear text. If the test is positive, it triggers two chains of action: one at the hospital and one at the lab.
At the hospital, the individual is registered in a centralized database and enrolled in a tele-health monitoring service at a COVID outpatient clinic for a 14-day isolation period. They will receive frequent phone calls from a nurse or physician who documents their medical and social history, and runs through a standardized checklist of 19 symptoms. All the data are logged in a national electronic medical record system. A team of clinician-scientists at the hospital created the collection system in mid-March with science in mind. “We decided to document clinical findings in a structured way that would be useful for research purposes,” says Palsson.
In the lab, each sample is tested for the amount of virus it contains, which has been used as an indicator for contagiousness and severity of illness. And the full RNA genome of the virus is sequenced to determine the strain of the virus and track its origin.
The same approach could work in other countries that have suitable resources, such as the United States, where all the methods deCODE is currently using were developed, says Stefánsson. In fact, early in the pandemic, many US labs pivoted to offer coronavirus testing, but were stymied by regulatory and administrative obstacles, which critics attribute to a lack of federal leadership. “This was a wonderful opportunity for academia in the United States to show its worth, and it didn’t,” Stefánsson says. “I was surprised.”
Viral fingerprints
Researchers at deCODE, the university hospital and the Directorate of Health began analysing the wealth of data in early March, and quickly published several early results. “Once we started to generate data, we couldn’t resist the temptation to begin to try to pull something cohesive out of it,” says Stefánsson.
Iceland’s COVID-19 results are limited by the fact that cases are occurring in a small and genetically homogeneous population compared with other countries, notes Palsson. But in some cases, that small sample size is also a strength, because it has led to detailed, population-wide data.
In early spring, most of the world’s COVID-19 studies focused on individuals with moderate or severe disease. By testing the general population in Iceland, deCODE was able to track the virus in people with mild or no symptoms. Of 9,199 people recruited for population screening between 13 March and 4 April, 13.3% tested positive for coronavirus. Of that infected group, 43% reported no symptoms at the time of testing2. “This study was the first to provide high-quality evidence that COVID-19 infections are frequently asymptomatic,” says Jade Benjamin-Chung, an epidemiologist at the University of California, Berkeley, who used the Iceland data to estimate rates of SARS-CoV-2 infection in the United States3. “It was the only study we were aware of at the time that conducted population-based testing in a large sample.”
A smaller population study, carried out in an Italian town, came to similar results on asymptomatic infection months later. When a 78-year-old man died in the northern Italian town of Vo’, Italy’s first COVID-19 death, the region’s governor locked the town down and ordered that its 3,300 citizens be tested. After the initial round of government testing, Andrea Crisanti, head of microbiology at the University of Padua in Italy, asked the local government whether his team could run a second round of testing. “Then we could measure the effect of the lockdown and the efficiency of contact tracing,” says Crisanti, who is currently on leave from Imperial College London. The local government agreed. On the basis of the results of the two rounds of testing, the researchers found that lockdown and isolation reduced transmission by 98%, and — in line with Iceland’s results — that 43% of the infections across the two tests were asymptomatic4.
In addition to tracking asymptomatic infections, the researchers in Iceland concluded that children under 10 were about half as likely to test positive as people aged 10 and older — a finding confirmed in Crisanti’s study of Vo’, as well as studies in the United Kingdom5 and United States6. Additionally, the deCODE team analysed the viral genetic material of every positive case, and used that fingerprint to track where each strain of the virus came from and how it spread. Most of the initial cases, the researchers found, were imported from popular skiing destinations, whereas later transmission occurred mainly locally, within families (see ‘Iceland’s three COVID waves’).
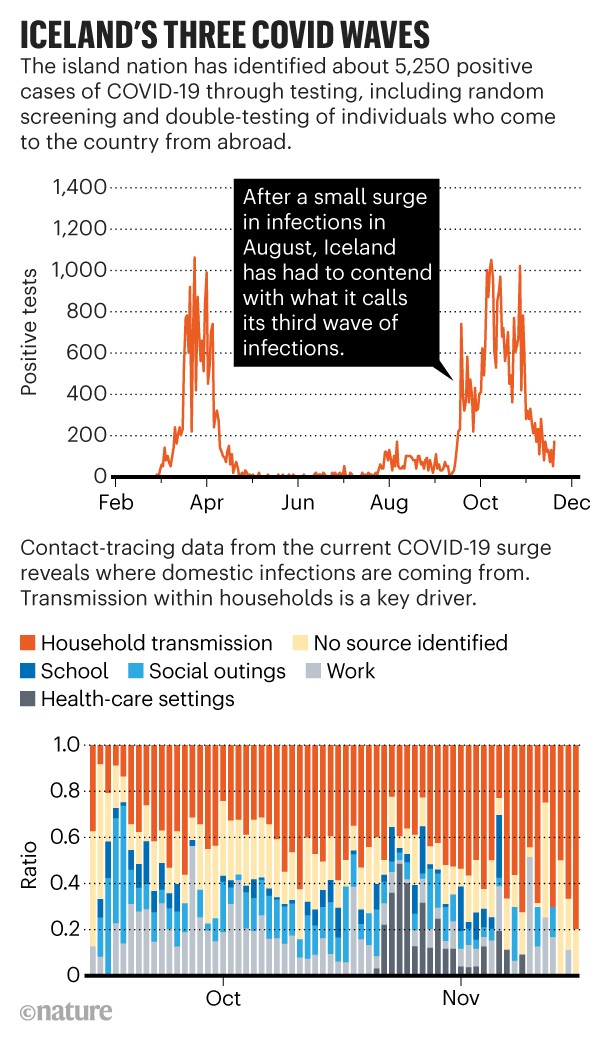
Source: http://www.covid.is/data; deCODE genetics
That genetic-tracing approach, called molecular epidemiology, was similarly applied in New Zealand to good effect. In March, New Zealand’s government implemented a stringent countrywide lockdown aimed at eliminating the virus. “Essentially, the New Zealand population more or less stayed at home for 7 weeks. After that, we emerged into a virus-free country,” says Michael Baker, a public-health researcher at the University of Otago in Wellington. That’s a feat for a country of 5 million people, more than 13 times larger than Iceland.
Genetic analysis of the first New Zealand wave, from March to May, showed that the strict lockdown began working right away. The rate of transmission — the number of people infected by each person with the virus — dropped from 7 to 0.2 in the first week in the largest cluster7. Sequencing data also showed that an August outbreak in Auckland, the source of which remains unknown, was from a single lineage, reassuring public-health authorities that there had only been one breach. “Genomics has played a vital role in tracking the re-emergence of COVID-19 in New Zealand,” says Jemma Geoghegan, a microbiologist at Otago who co-led the project with Joep de Ligt at the Institute of Environmental Science and Research in Porirua.
Getting the full picture
This summer at the university hospital, Palsson’s team used the clinical data to investigate8 the full spectrum of disease caused by SARS-CoV-2. The most common symptoms among the 1,797 people who tested positive between 31 January and 30 April were muscle aches, headache and a non-productive cough — not fever, a symptom listed in both the US Centers for Disease Control and the World Health Organization case definitions for COVID-19. When used to guide testing, those definitions are likely to miss some symptomatic people, says Palsson. “Hopefully others will come to a similar conclusion and that will result in changes in the criteria,” he says.
The results from Palsson’s team led to direct medical intervention in Iceland: individuals showing any sign of a common cold or aches are now encouraged to get tested, and the hospital categorizes new patients into one of three stages according to their symptoms, which dictates their level of care.
The most recent study from Iceland focused on a major COVID-19 question: how long does immunity to SARS-CoV-2 last? deCODE’s team found that anti-SARS-CoV-2 antibodies remained high in the blood of 91% of infected people for 4 months after diagnosis9, running counter to earlier results suggesting that antibodies decline quickly after infection10,11. It is possible that the conflicting results represent two waves of antibodies. In an editorial accompanying the paper12, Galit Alter at Harvard Medical School in Boston, Massachusetts, and Robert Seder at the US National Institutes of Health’s Vaccine Research Center in Bethesda, Maryland, suggest that a first wave is generated by short-lived plasma cells in response to acute infection, then a second wave, produced by longer-lived cells, bestows lasting immunity.
And finally, Stefánsson was able to pin down the elusive statistic that first intrigued him — the infection fatality ratio (IFR), or the proportion of infected people who die from the disease. Since the beginning of the pandemic, IFR estimates have ranged from less than 0.1% to a whopping 25%, depending on the size of the study and the age of the population. A growing number of studies are converging at about 0.5 to 1%. In Iceland, where the median age is 37 — relatively young compared with other wealthy nations — and patients have access to good health care, Stefánsson’s team found it to be 0.3%.
New wave
On 15 June, Iceland opened its borders to non-essential visitors from 31 European nations. A month later, on 16 July, the country also lifted restrictions on visitors from 12 more countries, including Canada, New Zealand and South Korea. The opening gave a boost to the struggling tourism industry, although numbers of visitors remained low, with about 75–80% fewer summer tourists than in 2019, according to the Icelandic Tourist Board.

Bars in Reykjavik reopened on 31 May, after a two-month closure.Credit: Haraldur Gudjonsson/AFP via Getty
Then, on 10 August, a pair of tourists at Reykjavik airport tested positive for SARS-CoV-2, ignored regulations and went into town. That incursion led to a small bump of cases in August centred on two pubs and a fitness centre visited by the tourists. Then, in mid-September, the number of infections increased abruptly, from 1 to 55 in a week. “This one clone of virus was able to spread around and cause lurking infections all over, especially in Reykjavik, and all of a sudden, we saw this increase,” says Guðnason. “It’s evidence of how difficult the virus is to contain.”
By October, coronavirus was more widespread in the community than it had been in the first wave, peaking at 291 infections per day. On 17 October, the number of active infections finally began to decline, which researchers attribute to widespread testing, tracing and quarantine procedures, as well as fresh government restrictions and emphasis on mask wearing. “Hopefully we can start relaxing our restrictions soon,” says Guðnason.
Despite the outbreak, the country continues to keep its borders open to tourists from some countries, although entry requirements are now stricter. Travellers must either self-quarantine for 14 days after arrival or participate in two screening tests: one on arrival, followed by five days of quarantine, then a second test. This method has led to the discovery that 20% of people who test negative in the first round will test positive in the second, notes Guðnason. That is a high number, but seems consistent with other analyses13. The new requirement is likely to have caught many strains of virus that would have otherwise entered the country.
Unlike New Zealand, which closed its borders, elimination was never supported in Iceland for fears that the country would go bankrupt without tourism. So it is possible that new cases will continue to arise, says Guðnason. Furthermore, he and others think the current outbreak might be in large part due to pandemic fatigue, as people disregard health precautions after months of being careful. “I think we’re going to be dealing with the virus, trying to suppress it as much as possible, until we get the vaccine,” he says.
And research continues in any and every spare hour. Palsson’s team is planning to analyse the effect of viral loads on patient outcomes and viral transmission, and to use contact-tracing data to tease out the risk factors for a super-spreading event. “We’ve had households where almost everybody gets infected, then other places where people carry the infection and stay in the workplace and nobody gets infected,” says Palsson. “It’s very difficult to understand.”
At deCODE, Stefánsson and his colleagues are investigating cellular immune responses and whether people with COVID-19 who are very sick produce antibodies directed against their own tissues. And together, the deCODE and university-hospital teams are collaborating on the long-term effects of COVID and how genetics affects susceptibility and responses to the disease.
“We’ve been committed for a long time to take everything we learn about human disease and publish it,” says Stefánsson. “There is no way in which we would have not utilized the opportunity.”
"how" - Google News
November 25, 2020 at 06:05PM
https://ift.tt/3nRzAzV
How Iceland hammered COVID with science - Nature.com
"how" - Google News
https://ift.tt/2MfXd3I
https://ift.tt/3d8uZUG
Bagikan Berita Ini














0 Response to "How Iceland hammered COVID with science - Nature.com"
Post a Comment